The most common locations for MCC are in areas of sun exposure on the face, neck and arms and head but they can occur anywhere on the body. While nearly all MCCs start on the skin, a very small number start in other parts of the body, such as inside the nose or oesophagus.
Symptoms & Diagnosis
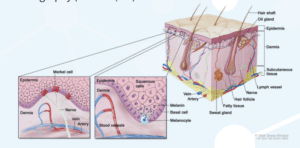
Merkel Cell Carcinoma often first appear as a single pink, red, or purple bump that is not usually painful.
Sometimes the skin on the top of the tumour might break open and bleed. As it’s appearance is similar to many other types of skin cancers, diagnosis is usually only made following a biopsy.
Clinical assessment for MCC can be remembered using mnemonic – AEIOU:
A – Asymptomatic
E – Expanding rapidly in less than 3 months,
I – Immunosuppression (lowered immunity),
O – Older than 50 years and
U – UV exposed locations on the body.
Treatment
MCC requires prompt treatment with treatment options varying depending upon whether the MCC is located in one area or has spread to other areas of the body.
Treatments used in MCC management include:
- Surgery
- Radiotherapy
- Chemotherapy
- Immunotherapy
MCC treatment is managed by medical specialists such as dermatologists, surgeons, radiation oncologists or medical oncologists.
Locoregional Disease Treatments
Merkel Cell Carcinoma Treatment Merkel cell skin cancer is rare, which means most doctors may not have seen or treated it before, so it is a good idea to get a second opinion on treatment options. After confirmation of MCC diagnosis, patients should be promptly referred to a specialist centre with experience in management of MCC.
Treatment options available include for “locoregional” disease (cancer is restricted to an area of the body):
Surgery
Surgery will usually involve an initial biopsy for diagnosis. Ongoing studies are recommending combined treatment methods to manage MCC which involves limited removal / biopsy (surgery) enhanced by giving radiation therapy after the operation.
Radiation Therapy (RT)
MCC is a highly radiosensitive tumour (which means the cells of the cancer react well to RT). Guidelines recommend RT be given following removal of the primary tumour. Radiation Therapy is a reasonable non-invasive alternative to resection in some patients. When removal of the tumour has taken place, studies have shown excellent local control rates with the addition of RT and there has been improvement in survival regardless of the tumour size. RT is also generally given to surrounding lymph nodes.
Aftercare
Ongoing surveillance includes regular skin examination and feeling of nodal areas and imaging with ultrasound, CT, or PET/CT.
Metastatic Disease Treatments
Treatment options for Metastatic Disease (cancer that has spread around the body):
Merkel Cell Carcinoma Treatment
MCC has a high risk of distant spread. National Comprehensive Cancer Network (NCCN) guidelines recommend patients with MCC which has spread around the body, to have systemic therapy (treat cancer cells wherever they may be) using chemotherapy or immunotherapy or combination of therapies such as systemic, resection and / or RT. Where possible, due to the advances in MCC treatments, patients should be considered for participation in clinical trials.
Chemotherapy
Chemotherapy is currently recommended in metastatic MCC for a palliative role (to control symptoms caused by MCC) and used when there has been failure of Immunotherapy to work, or if the patient has other health issues where Immunotherapy shouldn’t be used.
Radiation Therapy
Radiation Therapy is given when there is spread to reduce the symptoms (such as pain) in bone metastases or large lymph nodes. It can also help in altering the immune response. This is because MCC is very sensitive to RT and can reduce the size of the cancer, relieving symptoms and has very limited side effects at the doses needed.
Other Treatments
Treatments other than Immunotherapy are being studied for MCC patients who don’t respond to, or cannot have immunotherapy. Fifty to seventy percent of patients express somatostatin receptors (SSTRs) so somatostatin analogues are being investigated (for more information about somatostain analogues refer to NeuroEndocrine Cancer Australia website – Fact Sheet).
Peptide receptor radionuclide therapy (PRRT) is a novel approach which has a tumour-targeting peptide that delivers radiation to the cancer and spares the surrounding tissue. There are some studies combining PRRT and Immunotherapy being conducted.
Immunotherapy
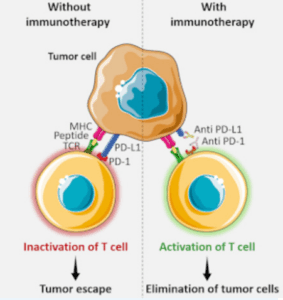
Immunotherapy is a treatment that uses the patient’s own immune system to fight cancer. Some types of immune cells, such as T cells, and some cancer cells have certain proteins, called checkpoint proteins, on their surface that keep immune responses in check. When cancer cells have large amounts of these proteins, they will not be attacked and killed by T cells.
Immune checkpoint inhibitors block these proteins and the ability of T cells to kill cancer cells is increased. These treatments take the ‘brake’ off your immune system to invigorate your immune system to re-recognise and fight the cancer (see Figure 1)
Currently immunotherapy is only available and approved for patients with advanced metastatic merkel cell carcinoma, but these treatments are being actively investigated in patients with earlier stage disease. There is currently a study open in Australia investigating this.
Clinical Trials – Support Services
Clinical Trials Melanoma and Skin Cancer Trials (MASC) provide information on current and closed trials, refer to this link: www.masc.org.au/content.aspx?page=trials
Current Trials which are recruiting are:
IMAT – A Merkel Cell Carcinoma trial for patients with Stage I – III. Treatment will be in combination with Radiation Therapy with Avelumab vs placebo for 6 months duration. The primary aim of the I-MAT trial is to develop an effective, well-tolerated combination regimen including immunotherapy for patients with stage I-III MCC. Trial link: https://clinicaltrials.gov/ct2/show/NCT04291885
Gotham – Targeted Therapy and Avelumab will investigate anticancer activity for combination of Avelumab plus Peptide Receptor Radionuclide Therapy (PRRT) and Avelumab plus Radiation Therapy (RT) in patients with unresectable or metastatic MCC. Trial link: https://clinicaltrials.gov/ct2/show/NCT04261855
Support Services
NeuroEndocrine Cancer Australia: neuroendocrine.org.au
Amigos: amigos.org.au
References
www.cancer.gov/types/skin/patient/merkel-cell-treatmentpdq Oct 2019
Kok DL, Wang A, Xu W et al. The changing paradigm of managing Merkel cell carcinoma in Australia: An expert commentary. Asia-Pac J Clin Oncol. 2020;108.
https//doi.org/10.1111/ajco.13407
neuroendocrine.org.au/wp-content/uploads/2020/07/N5058- NECA_SSAInfo_Download-v1.pdf
